
From the 1Roessingh Center for Rehabilitation, 2Roessingh Research and Development, 3Medisch Spectrum Twente, 4University of Twente, Enschede, The Netherlands. *These authors contributed equally to this work.
Objective: To evaluate the effectiveness and safety of intrathecal baclofen treatment of spasticity, administered via a cervical catheter tip.
Design: A review of PubMed and the Cochrane Library up to September 2020. No restriction in study design. Two reviewers independently evaluated eligibility, extracted data and evaluated risk of bias. Studies were included in which patients were treated with intrathecal baclofen for spasticity, with the catheter tip at or above the first thoracic level, independent of diagnosis and age.
Results: Thirteen studies were eligible, with a moderate to critical risk of bias. Improvement in spasticity was seen only in the upper extremity in 6% of subjects, only in the lower extremity in 2%, in both upper and lower extremities in 50% and without specification of location in 41%. Upper extremity function improved in 88% of cases. Neither drug-related (1%) nor technical (21%) complications occurred more often than in lower placement of the tip. Effects on respiratory function and sleep apnoea were not investigated.
Conclusion: Cervically administered intrathecal baclofen seems to improve upper extremity spasticity and function, without causing more complications than thoracolumbar intrathecal baclofen. However, the mainly drug-related complications have not been thoroughly investigated and the available literature is of poor methodological quality. Further research is needed to confirm the efficacy and safety of this procedure.
Key words: intrathecal baclofen; tip placement; cervical; upper extremity; spasticity.
Accepted Jun 16, 2021; Epub ahead of print Jun 23, 2021
J Rehabil Med 2021; 53: jrm00215
Correspondence address: Nora W. Jacobs, Roessingh Center for Rehabilitation, Enschede, The Netherlands. E-mail: n.jacobs@roessingh.nl
Doi: 10.2340/16501977-2857
Spasticity is a common complication in central neurological disorders. It can lead to discomfort and functional limitations. To reduce spasticity, administration of baclofen via a catheter into the spinal canal has been used successfully for several years. However, this treatment often has limited effects on the upper limbs. The catheter tip is often situated in the thoracolumbar region. This review suggests that baclofen treatment via a cervically located catheter tip reduces spasticity of both arms and legs. Also, arm function improved in patients with a cervical catheter tip. Neither drug-related nor technical complications occurred more often than in lower placement of the cervical catheter tip. Few studies were found on this subject, and the available literature is of poor quality. Therefore, more research is needed to confirm the positive effect of this procedure on spasticity of the arms and to monitor for complications.
Spasticity is a common complication after central nervous system injury with involvement of the upper motor neuron. The prevalence varies from 45% in stroke, 65% in spinal cord injury to 80% in multiple sclerosis (1–3).
Spasticity is most commonly defined as “velocity-dependent increase in the tonic stretch reflex”, but has been redefined in 2005 by the European working group EUSPASM as “disordered sensori-motor control, resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles” (4, 5). Depending on the severity, spasticity can negatively influence voluntary movement and lead to discomfort and functional limitations (5, 6).
In functionally limiting spasticity, non-invasive treatment options, such as elimination of spasm provoking stimuli and physical therapy, should be considered first. In case of insufficient effect, oral medication can be started for general spasticity, or botulinum toxin, phenol or surgery for focal spasticity (7). Baclofen is the most commonly used oral antispasmodic (8). It is a centrally-acting gamma aminobutyric acid (GABA)-B agonist that works as muscle relaxant by diminishing reflex transfer at the spinal cord level. As orally provided baclofen poorly crosses the blood–brain barrier, high doses may be needed to achieve a functional effect, which may induce side-effects, such as fatigue, respiratory depression and confusion. Baclofen can also be administered locally via an intrathecal catheter, resulting in fewer side-effects than systemic baclofen treatment (6). The lower occurrence of side-effects can be explained, on the one hand, by a lower required baclofen dose (as the blood–brain barrier no longer has to be crossed), resulting in fewer general side-effects, and, on the other hand, by a lower cerebral baclofen concentration, resulting in fewer central nervous side-effects.
The effect of intrathecal baclofen (ITB) on spasticity of the lower extremity (LE) has been well described in numerous studies, whereas the effect on spasticity of the upper extremity (UE) is less certain (9, 10). This difference in effectiveness might be related to the position of the intrathecal catheter tip and the baclofen gradient in the cerebrospinal fluid. The catheter tip is often positioned at the thoracic or lumbosacral level, assuming that the cerebrospinal fluid flow distributes baclofen in the intrathecal space to the required site of action. However, 2 studies that have been conducted on ITB distribution in humans show a steep concentration gradient of baclofen (11, 12). Kroin et al. found a lumbar-to-cisternal decrease in concentration of approximately 75% (11), and Heetla et al. reported a decrease in concentration from T10 to 30% at 5 cm tip distance, 12% at 10 cm and 0.7% at cerebral level (12). This baclofen concentration gradient suggests that, for optimal treatment of UE spasticity, the catheter tip should be located at the high thoracic or cervical level.
Balsara et al. and Albright et al. suggest that catheter tip position should be dependent on treatment goal: T10–12 for diplegia and C5–T2 for tetraplegia (8, 13). However, in clinical studies there is no consensus on the relationship between catheter tip position and the effect on spasticity (14, 15).
The demand for adequate treatment of UE spasticity has increased, as there is a growing number of patients with cervical spinal cord injury (16–18). A cervically positioned catheter tip could ameliorate spasmolytic effects on the UE due to higher cervical concentration of baclofen. However, it might lead to an insufficient effect on LE spasticity. Cervical ITB could also influence respiratory function and sleep-related disorders, either positively or negatively (19–21). Furthermore, a high cervical concentration of baclofen could increase cerebral side-effects and thereby influence cognitive and emotional functions. In this systematic review, the effectiveness and safety of baclofen treatment via a cervical catheter tip is analysed.
Search strategy
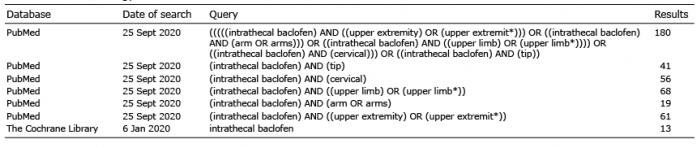
A literature search in PubMed and The Cochrane Library was conducted to find relevant English or Dutch articles, without a restriction on publication period or study design. Key words used were “intrathecal baclofen”, “upper extremity”, “arm”, “upper limb”, “cervical” and “tip” (Table I). Reference lists were checked for eligible studies. Trial registers (Prospero, ClinicalTrials.gov, www.trialregister.nl) were searched for ongoing trials.
Table I. Search strategy
Study selection
Studies were included in which patients with spasticity were treated with ITB, with the catheter tip at a cervical vertebral level or at the first thoracic vertebral level. Inclusion was independent of diagnosis and age, because of the limited studies available on cervical ITB. Reviews were excluded because none of them specifically described the effect of cervical ITB. Prior to exclusion, the reviews were checked for relevant references, which were added to the screening list for eligibility in the current review. Also, relevant references of the other included studies were added to this screening list. Two reviewers (NJ, EM) independently examined study eligibility. In case of unknown catheter tip height (n = 21), authors were asked for information about catheter position by e-mail, with a reminder after 2 weeks. Three reactions were received: 2 studies concerned low tip placement, in one study tip location was unclear. The low response is probably due to dated studies: 18 of 21 studies with unknown tip height were published before 2015. The author of a study in which only one participant received cervical ITB was requested to send specific information regarding this case; however, no reaction was obtained and the study was excluded (22). Also, specific outcomes regarding the cervical ITB patients (n = 9, total n = 166) in a study was requested, without response (14). Therefore, this study was also excluded. Three studies were added to the review via references. Of these studies, one was not available in the databases searched (23), and the other 2 did not focus on upper limb function (24, 25), which explained why they were not selected using the key words used in the current study.
Data collection and analysis
Two reviewers (NJ, EM) independently assessed risk of bias of the selected studies and extracted data regarding study design, intervention details, number of participants, intervention details and outcomes (spasticity, UE function, complications, additional findings). In case of disagreement, a third reviewer was involved in the discussion (MB). Risk of bias was evaluated as low, moderate, serious or critical, using the ROBINS tool for the cohort study and the tool developed by Murad et al. for case reports and case series (26, 27).
Measurement scales
The following scales were used in the selected studies:
Description of studies
Thirteen eligible studies were found (Fig. 1): 1 cohort study (15), 11 case series (23–25, 31, 36–42), and 1 case report (43). There were no randomized controlled trials on cervical ITB. No ongoing trials were found in trial registers. In total, 121 patients with a tip at or above vertebral level T1 were included. Risk of bias was moderate in 5 (15, 23, 40–42), serious in 6 (15, 25, 31, 36–38, 43) and critical in 2 (24, 39) studies (Appendix 1 and Appendix 2). Risk of bias of the study of McCall & MacDonald was evaluated for 2 different outcomes: it was moderate for Ashworth and serious for complications (15). Study characteristics and outcomes are shown in Table II.
Fig. 1. Study selection.
Table II. Study characteristics and outcomes
Description of results
Spasticity. Spasticity was evaluated in 9 studies (15, 24, 25, 31, 36–38, 40, 43). In total, the effect of cervical ITB on spasticity has been described in 54 patients. In all but one patient, improvement was reported. This concerned improvement only in UE spasticity in 3 cases (6%), mixed improvement in UE and LE spasticity in 27 cases (50%), improvement in only LE spasticity in 1 case (2%), and spasticity improvement without specification of location in 22 cases (41%). In the only patient without improvement, a stable tone was reported with cervical ITB treatment.
Spasticity was most often evaluated using the (modified) Ashworth scale. All 6 studies that used AS/MAS reported a lower score with ITB treatment: MAS score improved from 2–4 without ITB to 0–3 with ITB (36, 40, 41); AS improved from 3–5 to 1–3.1 (15, 25, 31). SPS improved in both studies in which it was evaluated: range from 0–4 before treatment to 0–1 after treatment (25, 31). Also, RF improved: from 3–5 before start of ITB to 2–3 with ITB (25, 31). Four studies described a subjective improvement in tone or spasticity control (24, 36–38). Spasticity did not become worse in any study.
Six studies specifically reported spasticity effects on UE (15, 24, 36, 37, 40, 43). Aljuboori et al. described UE tone improvement in 2 cases and a stable tone in the other 2 cases, of which 1 showed LE tone improvement (37). The other studies mentioned only positive effects: MAS improved from 2–4 without ITB to 0–3 with ITB (15, 36, 40, 43) and subjective tone improvement was noted (36, 25).
Four studies compared changes in spasticity effects on UE and LE (Table II) (15, 36, 37, 40). In 2 patients improvement in UE tone occurred, without change in LE (36, 37). One patient showed improvement only in LE tone (37). In most patients however, spasticity of both UE and LE improved with ITB treatment (15, 37, 40). In these studies Aljuboori et al. did not quantify the degree of improvement in tone (37). Hamed et al. described MAS improvement from 3–4 in UE and LE before ITB to 0–3 in UE and 1–2 in LE after ITB (40). McCall and MacDonald found a significant improvement on the AS for both UE (4.0 (SD 0.8) to 3.0 (SD 0.9)) and LE (4.0 (SD 0.9) to 3.1 (SD 1.0)) with cervical ITB treatment, whereas their thoracic tip control group showed only a significant difference on LE (3.5 (SD 0.7) to 2.3 (SD 1.2)) (15). Improvement in UE AS (2.6 (SD 1.5) to 2.1 (SD 1.2)) was not significant in the thoracic group.
Upper extremity function. Six studies reported an effect of the ITB treatment on UE function (Table II) (23, 24, 36, 37, 41, 42), describing a total of 33 patients. UE function improved in 29 patients (88%), remained stable in 3 (9%), and worsened in 1 (3%). Only one study used a scale (MUUL) to demonstrate the effect, which was positive: dominant limb score improved from 46.42 (SD 19.6) to 55.44 (SD 17.4) (41). Other studies noted subjective positive effects on handwriting, dressing, bringing hand to mouth and driving a powered wheelchair (36, 37, 42). One study reported improvement in 15 patients, but unchanged function in 3 patients and worsened function in 1; specification of these effects was not reported (23).
Complications. Complications of the cervical ITB treatment were divided into 2 groups: drug-related (i.e. side-effects of baclofen) and non-drug-related (other adverse events, such as pump and/or catheter-related problems or infection).
In all but 2 studies included in this review (36, 40), complications were reported. This concerned a total of 116 cases. Only 1 case with drug-related complications was reported (1% of the 116 included cases) (15). However, Chappuis et al. found that somnolence and urine retention were the most seen complications, although without reporting the number of cases (24). The reported drug-related case concerned somnolence leading to aspiration pneumonia (15). The somnolence was related to the use of both cervical ITB and oral baclofen and improved after discontinuation of oral baclofen without change in ITB. Two studies explicitly denied respiratory depression; however, they did not mention testing this complication (31, 41).
Non-drug-related complications occurred more often: they were reported in 8 studies, involving a total of 24 cases (21% of the 116 patients with reported complications). Most common were catheter fracture (n = 5, 4%), infection (n = 5, 4%) and cerebrospinal fluid leakage (n = 5, 4%).
Other outcomes. Several other effects of ITB treatment were observed (Table II). Subjective functional improvements were seen in gait (n = 6), ease of (self-)care (n = 31) and speech and/or swallowing (n = 4) (23–25, 31, 36–38, 40, 41). Also, mood (n = 10) and level of consciousness (n = 5) ameliorated (23, 25, 31, 36).
One study stated a preserved contralateral and/or LE function in unaffected extremities (40). Chang & Ehsan reported improvement in motor strength in UE in one case from 2–3/5 to 4/5 (36).
Dystonia was assessed in 3 studies, using the BAD, BFM, TWSTRS, and a patient and caregiver questionnaire (23, 41, 42). Improvement was seen in all dystonia evaluations.
ITB via a thoracolumbar catheter is an effective and safe treatment for LE spasticity (9). However, it often has limited effects on the upper limbs (44–46). This review suggests that baclofen treatment via a cervically located catheter tip reduces spasticity and improves function of the UE without causing more complications, but confirmatory research is needed because of the moderate to poor methodological quality of the current studies.
Studies
This literature search found few studies on cervically administered ITB. Most studies have a low level of evidence: 11 case series (23–26, 31, 36–42), 1 case report (43). One retrospective cohort study was included (15). All studies had moderate to critical risk of bias. Common and important risks of bias were inadequate ascertainment of outcome, insufficient evaluation of co-interventions, and insufficient reporting of research procedure. No randomized controlled trials have been published on this subject. Moreover, the available studies do not answer all our questions. Complications were often described in a limited way, without specific evaluation of respiratory function, sleep-related disorders, effects on cognitive or emotional function or gait. Regarding efficacy, only 9 studies described effects on spasticity (15, 24, 25, 31, 36–38, 40, 41). Three studies concerned cervical ITB in patients with dystonia (23, 41, 42) and one study focused on surgical aspects of cervical catheter placement, rather than the effect on spasticity (39). Six studies evaluated effects on UE function (23, 24, 36, 37, 41, 42). To describe efficacy, different measurement tools were used, which complicated comparison of the studies. With the currently available data, it is impossible to perform a meta-analysis.
Pharmacodynamics in intrathecal baclofen
The effect of ITB on spasticity of the LE has been described in numerous studies, whereas the effect on the UE seems to be less certain (9). This difference in effectiveness might be related to the steep baclofen gradient in the cerebrospinal fluid. The ITB gradient has been demonstrated in 2 studies, in which baclofen was administered at L3 and T10, with concentrations dropping to 24% at cisternal level and 0.7% at cerebral level, respectively (11, 12). The catheter tip is often positioned in the thoracic and lumbosacral level and consequently, baclofen concentration at the cervical region could be too low to cause spasmolytic effects on the UE (9, 47).
Factors that contribute to ITB drug distribution are infusion rate and location of infusion. Concerning infusion rate, a lumbar quick bolus raises cervical concentration more than lumbar slow continuous infusion (47, 48). To achieve maximal distribution, a low concentration of baclofen could be administered at a fast infusion rate. The disadvantage of this is that the pump empties quickly. As regards infusion location, it is important to know that cerebrospinal fluid flows rapidly at the cervical region, whereas there is hardly any flow at the lumbar level (49). Therefore, lumbar-administered baclofen is less likely to distribute towards the cervical spine, whereas cervical administration will probably lead to wider distribution.
Spasticity
Based on the steep concentration gradient of ITB, as demonstrated by Kroin et al. and Heetla et al. (11, 12), it was expected that cervically administrated baclofen would lead to better control of UE spasticity. However, with cervical administration, effect on LE spasticity might be insufficient. This was not confirmed in this review: in most patients both UE and LE spasticity improved (15, 36, 37, 40). The effect on LE despite administration at a high intrathecal level might be explained by the faster cerebrospinal fluid flow at cervical region compared with the flow at lumbar level (49), which causes high baclofen concentrations at greater tip distance.
Only one study evaluated effect differences between cervical and thoracic tip placement: improvement in UE and LE spasticity was seen with a cervical tip, whereas only LE spasticity improved with a thoracic tip (15). This finding fits the assumption that thoracically administered baclofen causes too low cervical concentrations and therefore does not act on the UE. However, this is a retrospective study with a moderate risk of bias in spasticity measurement.
Upper extremity function
An important reason to treat UE spasticity is functional limitations. It was expected that better control of UE spasticity would lead to a functional amelioration. All included studies that assessed UE function stated functional improvement with cervical ITB treatment (23, 24, 36, 37, 41, 42). One study reported deteriorated function in one patient, without further specification (23). Only one study used a scale to measure functional improvement, which demonstrated improvement on the MUUL from 46.42 (SD 19.6) to 55.44 (SD 17.4) (41). However, an improvement of at least 14 points on the MUUL scale is needed to reflect a true change in function (minimal clinically important difference) rather than an error in measurement (32). The subjective improvement reported in multiple studies suggests a positive effect of cervical ITB on UE function, although objective research is needed to confirm this effect and to specify the degree of improvement.
Complications
According to the literature, ITB causes drug-related side-effects in 4.4–54% of patients, most commonly drowsiness, dizziness, constipation and hypotonia (50, 51). Also, brainstem effects have been reported, e.g. respiratory depression, hypotension, bradycardia and coma (51). Other central nervous side-effects include confusion and psychological symptoms (6, 9). The catheter tip is usually placed at the lumbothoracic level, because it is thought that higher tip placement raises the concentration of baclofen at the brainstem and cerebral level and thereby reduces central nervous side-effects (6, 9).
In this review, drug-related complications were reported in 1% of all cases. This is less than reported in other literature (50), possibly due to more careful titration due to fear of side-effects with a cervical tip, or due to insufficient registration of side-effects. Moreover, Chappuis et al. reported urine retention and somnolence in an unknown number of cases (24). Because of the unknown number of cases, this could not be included in the calculated percentage of complications.
The reported somnolence could be explained by co-administered oral baclofen in the titration phase of the ITB; after discontinuation of oral baclofen mental status improved (15). In this study, no drug-related events were reported in the thoracic ITB group. Regarding respiratory function and sleep-related disorders, cervical ITB might influence either positively, due to reduced spasticity of thoracic muscles, or negatively, due to central side-effects or peripheral muscle weakness. Previous research demonstrated positive effects of continuous thoracic ITB on respiratory function (21); however, also a worsening of sleep apnoea syndrome on boluses (20). The current review found no reported effects on respiratory function and sleep apnoea syndrome.
Another theoretically possible complication of ITB is deterioration in gait function due to reduced LE strength. This particularly involves patients with spasticity of the UE and preserved LE function, such as in central cord syndrome. The unwanted effect of ITB on the LE could occur despite cervical tip placement, as LE spasticity can be treated using cervical ITB, as mentioned above. In this review, gait improvement was reported; however, this concerned cases with LE spasticity (25, 31, 37, 40). The ITB effect on gait function in patients with only UE spasticity remains unknown. Since no weakness or function loss was observed on the healthy contralateral side (40), a limited negative effect of cervical ITB would be expected, although confirmatory studies are needed.
Non-drug-related complications happened more often than drug-related problems, which is also the case in lower positioned ITB (9). Technical complications might happen more often in cervical ITB, due to the long intrathecal part of the catheter, which could increase risk of migration and fracture (6). However, McCall & MacDonald found no relation between tip height and technical complications (15). In this review, 21% of patients had a non-drug-related complication; according to the literature this occurs in 20–36% of patients with ITB treatment (50). To prevent a long intrathecal catheter, a C1–2 entry site could be an alternative for the traditional lumbar entry site (37). This might be particularly useful in patients with (future) scoliosis correction, since the entrance at vertebral level C1–2 ensures that the ITB catheter does not cross the surgical region of the thoracolumbar vertebrae and the thoracolumbar spinal canal.
This review shows that ITB administered via a cervically located catheter tip results in improvement in UE spasticity and function (15, 23, 24, 36, 37, 40–43). Cervical tip placement has shown to be more effective to treat UE spasticity than a thoracic tip placement (15). Also LE spasticity improved with cervical ITB (15, 36, 37, 40), possibly due to the faster cerebrospinal fluid flow in the cervical region compared with the lumbar level, which causes higher concentrations of baclofen at greater distance from the tip. The effects on gait remain unknown.
The higher cervical concentration does not seem to cause more drug-related complications; however, this has not been thoroughly investigated. Effects on respiratory function and sleep apnoea mainly remain unknown. Technical complications do not occur more often in patients with a cervical tip placement.
The available literature is of a low level of evidence and has a high risk of bias. Therefore, more research is needed to confirm the efficacy and safety of cervically administered ITB.
Appendix 1. Risk of bias of included case series and case reports, evaluated according to Murad et al. (27)
Appendix 2. Risk of bias of the included cohort study, evaluated according to ROBINS-I (26)


 Click to show fullsize
Click to show fullsize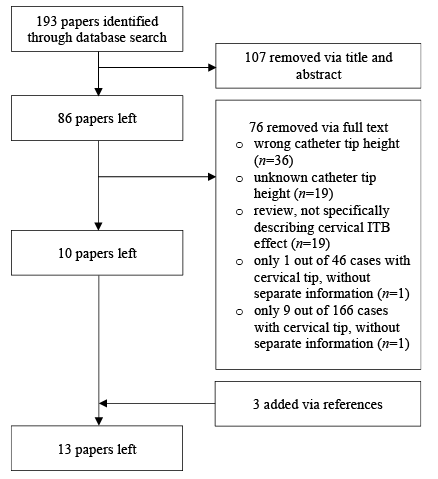 Click to show fullsize
Click to show fullsize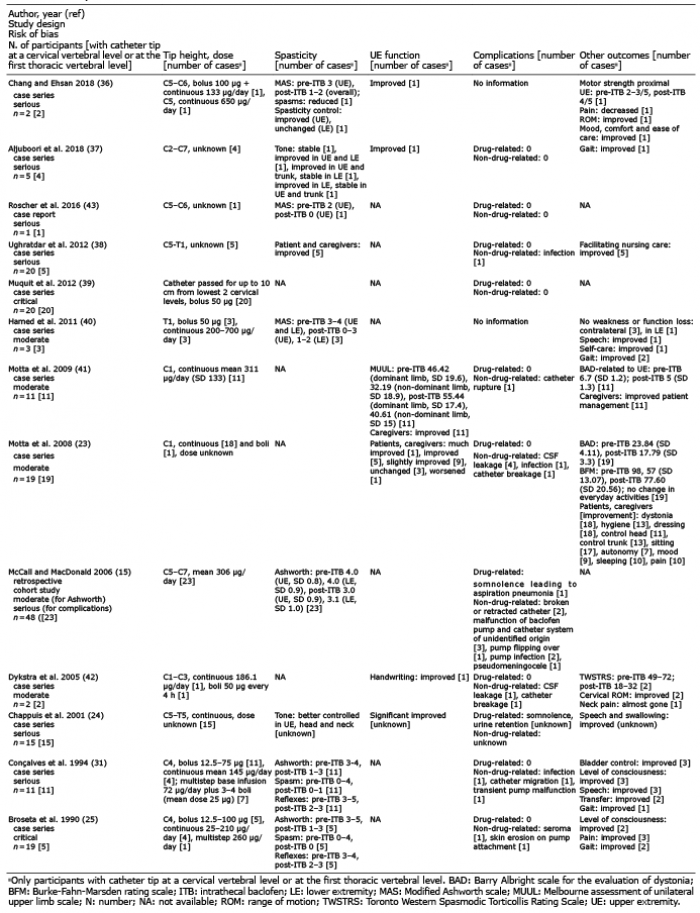 Click to show fullsize
Click to show fullsize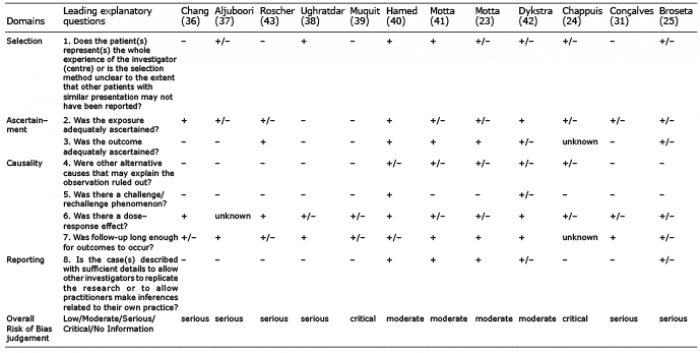 Click to show fullsize
Click to show fullsize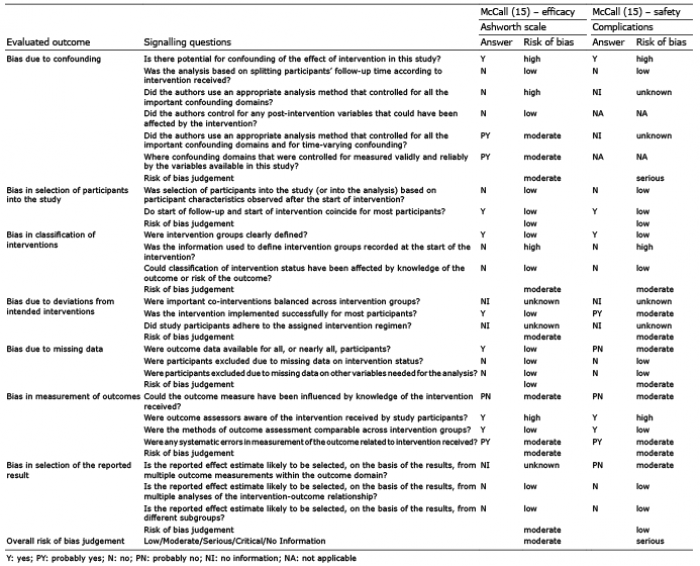 Click to show fullsize
Click to show fullsize